Before and after photos on supraeruption of teeth and tooth hypereruption performed in our Braces Orthodontics office.

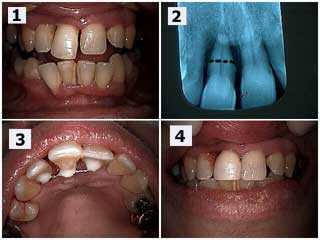
The lower front tooth had supraerupted because of severe periodontitis (gum disease) and exhibited complete bone loss in the x-ray. A splint made of orthodontic wire and composite bonding was placed behind these lower front teeth and then the biting edge of this tooth was adjusted to make it even with the adjacent teeth. Then the apical (lower) half of this tooth was resected (cut) and then extracted leaving the remaining half intact within the splint (see x-ray). Composite Resin Bonding was then placed between the teeth to hide the wire splint from a front view. Lastly, the broken two upper front teeth were bonded.

A Russian investment banker came from Moscow for fast and esthetic replacement of an upper front broken tooth. Understanding the etiology of the fracture, and treating it, will help prevent recurrence. In this case, the supraeruption of the lower front teeth need incisal adjustment and then removable orthodontic retention.
How to treat supraeruption of a loose upper front tooth. Photo 1) The upper right central incisor #8 has supra-erupted resulting in a diastema – gap space. 2) The x-ray shows severe bone loss but this patient wanted to try to keep this tooth for as long as possible. The black dotted line shows the location for a potential root resection if necessary. Root planing was performed after a teeth splint was placed. The patient will return in three months to reevaluate periodontal healing with the Periodontist and the potential need for the root resection. 3) Palatal photo of the dental splint between teeth #’s 7 – 9. 4) Post-op photos taken on the same day. Notice the diastema space was closed with bonding to hide the splint and the incisal edge of #8 was reduced.

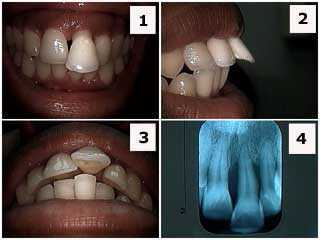
Supraeruption is commonly seen in upper front teeth where there is periodontal gum disease and a traumatic occlusion – bad teeth bite. How to treatment of supra-eruption for a maxillary central incisor #9. 1) & 2) Pre-operative photograph and radiograph. Note the angular bony defect in the x-ray. The patient reported that the tooth was getting longer and that he never previously had the gap space between his two front teeth. This patient was also a smoker. 3) Palatal photo of the extracoronal teeth splint placed between teeth #’s 8 & 9. 4) Post-operative image one hour later. Teeth bonding was placed to close the space also hides the palatal splint. The incisal edge of #9 was shortened and the occlusion teeth bite was checked and adjusted for fremitus – tooth vibration upon closing. Root planing was next performed and the patient placed on a three-month periodontal reevaluation.
Diagnosis of the etiology of supraeruption. This patient was only in her 20’s but she already had significant periodontal gum disease. 1) Front photo. 2) Side photo. 3) Occlusal picture. 4) Xray. The patient was informed about the severe periodontal condition and that the prognosis for this tooth was poor. She was informed that a thorough check-up with a Periodontist was recommended. Orthodontics teeth braces is contra-indicated here because of the severe periodontal gum problem. If the patient wants to try to maintain this tooth as long as possible then treatment could include: scaling and root planing, open flap debridement if necessary, root canal therapy and dental crown (for esthetics) and possibly a teeth splint. Treatment, otherwise, could just include scaling and root planing and incisal adjustment. I have found that many patients prefer to ease into the idea of an extraction of a front tooth since it can be very emotionally traumatic.

Supraeruption occurs when a tooth continues to grow out of the gum if the opposing tooth in the opposite jaw is missing. Treatment involves placing a tooth in the missing space and adjusting the height of the supra-erupted tooth.