Photos and X-rays on cleaning and shaping in root canal or endodontics created in our Root Canal office.
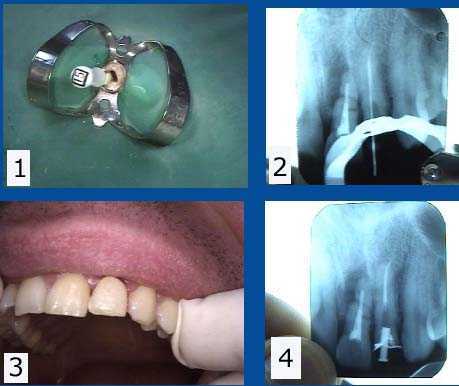
Endodontist root canal retreatment of an upper left lateral incisor following fracture of an old crown. (The adjacent central incisor #9 will need to be extracted due to apical fracture). 1) Tooth #10 (upper left lateral) canal widened with an endodontic file. Old gutta percha removed using Chloroform solvent. A rubber dam clamp and rubber dam in place on the tooth to maintain sterility. 2) Radiograph of an endo file marker used to measure vertical depth of root canal to apex. The prior gutta percha was not obturated to the canal apex and the gutta percha had been left exposed to saliva after the crown fracture. 3) Root canal filled with new gutta percha, temporary crown and temporary post re-inserted. 4) Post-op radiograph showing the obturated root canal and post space in preparation for a cast gold post and core impression.
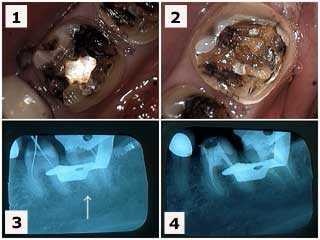
1) & 2) Tooth #’s 19 & 18 following removal of large, old silver fillings in a 38 year-old female patient who had been experiencing root canal pain. 3) Endodontist X-ray of endodontic file lengths. Note that the calcification in the mesial root of #18 initially prevented instrumentation. 4) Final endodontic obturation showing that the mesial root of #18 was located and treated. Chronic inflammation in the dental pulp due to the presence of large, old fillings can increase the difficulty of root canal therapy. Earlier root canal therapy should be considered in these situations.
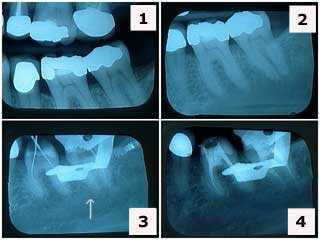
1) & 2) X-rays of tooth #’s 19 & 18 showing large, old silver fillings in a 38 year-old female patient who had been experiencing root canal pain. Note the decreased size of the pulp chambers in these teeth. 3) X-ray of endodontic file lengths. Note that the calcification in the mesial root of #18 initially prevented instrumentation. 4) Final endodontic obturation showing that the mesial root of #18 was located and treated. Chronic inflammation in the dental pulp due to the presence of large, old fillings can increase the difficulty of root canal therapy. Earlier root canal therapy should be considered in these situations.
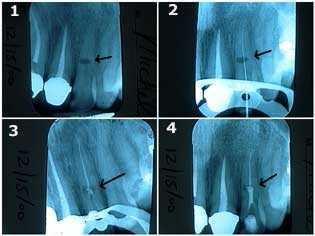
Treatment of internal resorption in an upper left lateral incisor. This 40-year-old female related a history of trauma to her front teeth during a horseback riding accident. 1) The oval-shaped radiolucency in the middle of the tooth length is the site of the internal resorption. The patient was informed of the guarded long-term prognosis of the tooth. 2) & 3) Traditional root canal therapy was first performed. The canal space was cleaned and shaped, sterilized with NaOCL, and then filled with gutta percha up to a point apical to the internal resorption. 4) MTA, Mineral Trioxide Aggregate, was then placed into the area of the internal resorption and coronal to it. Keeping the MTA moist will give more working time for condensation of material. [Thanks to Dr. Michael Collura for technical assistance.]
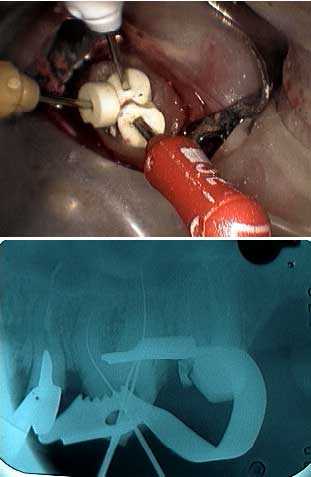
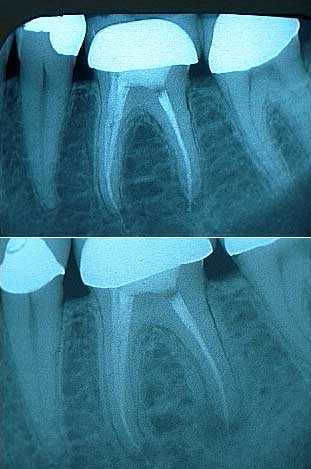
Three endodontic files are placed in a maxillary molar by the Endodontist to verify the correct lengths in the radiograph. How to root canal therapy pictures.

Endodontic technique in an upper left canine. 1) The file is placed within the canal by the Endodontist prior to the measurement radiograph. 2) Lateral condensation after the master cone is cemented. 3) and 4) Heating the endodontic condenser to vertically condense and sever the gutta percha at the pulpal chamber floor. How to root canal therapy pictures.
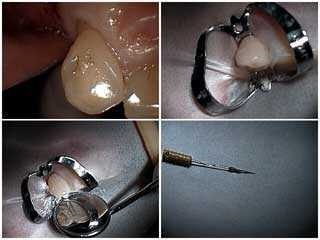
1) Endodontic technique in an upper left canine. 2) The tooth is surrounded by a rubber dam and a butterfly clamp. 3) This Endodontist mirror view shows the obturated root canal. 4) The extirpated root canal pulpal tissue is shown.
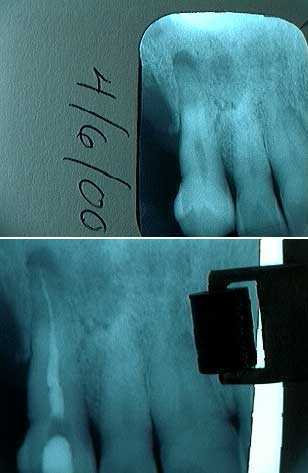
Root Canal Diagnosis x-rays: 1) Tooth #11 pre-operative film showing the periapical pathology. 2) The final radiograph shows the gutta percha reaching the apex of the tooth root.
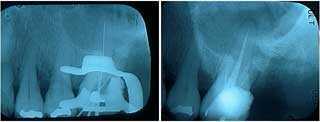
X-rays of root canal therapy showing initial lengths and then final obturation in an upper left first molar of a 40 year-old female. Obturation is the placement of root canal filling material by the Endodontist.

Comparison of the initial and final radiograph of root canal retreatment of a maxillary second premolar. The root canal filling material does not reach the apex of the tooth root in the initial x-ray but now does in the final radiograph. It is better for patients to have an Endodontist perform root canal therapy to minimize the need for retreatment.

Root canal retreatment performed by an Endodontist. 1) Endodontic access is attained after removing old filling material. 2) The measurement file is placed. 3) The measurement radiograph shows the file reaching the apex of the tooth root. This gives an accurate measurement of the canal length. 4) The canal is filled with gutta percha.
Before and after x-rays of a retreated molar root canal. 1) The post op radiograph of the initial root canal looks good. A little root canal dental cement can be seen extruding from the apices. 2) A two year follow up radiograph showed the development of an expanding periapical radiolucency. This second view shows the retreated molar and the periapical radiolucency at the time of the retreatment. Dental patients should seek out an Endodontist to perform root canal therapy to decrease the chance they will need retreatment.