Photos and X-rays on X-rays of root canal therapy include PA radiographs created in our Root Canal office.
Digital dental x-rays of a Dental Reconstruction Oral Rehabilitation. An initial panoramic radiograph xray and two midtreatment periapical xrays are shown with pictures. This patient did not have tooth pain symptoms!
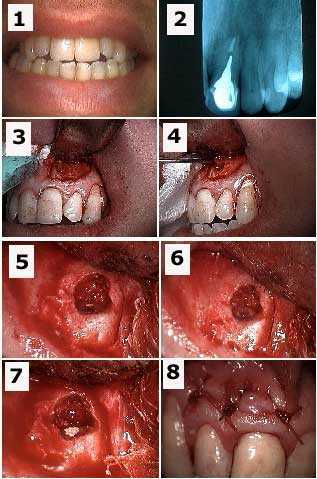
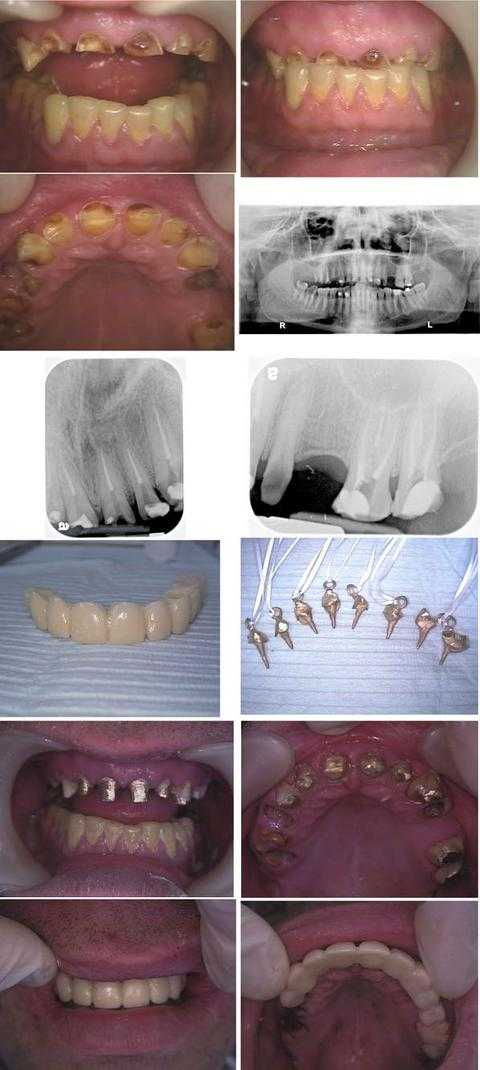
Dental Reconstruction of a phobic Wall Street executive. Total treatment time was about nine hours in two visits during one business week: Monday (four hours) and Friday (five hours). This patient hid his dental condition for over a decade by refusing to smile.
In the first row of photos, note that the teeth bite occlusion was over-closed due to a prior history of an eating disorder, now controlled, and a current teeth grinding habit called bruxism.
An Oral Surgery consultation with a digital panoramic x-ray (second row) was performed prior to treatment to evaluate opening the teeth bite.
The third row shows dental x-rays taken after the Endodontist completed root canal treatment on eight teeth on the first day on tooth #’s: 6 – 11 and 14, 15.
The fourth row shows the lab-processed 11 unit – 11 teeth – temporary dental bridge and the cast gold post and cores with Kaitlyn loops for the root canal treated teeth.
The fifth row shows the cast gold post and cores cemented.
The sixth row shows the lab-processed temporary dental bridge in place after the Oral Surgeon extracted tooth #’s: 3 – 5 and 12, crown lengthening gum surgery was performed on tooth #’s: 6 – 11, and a distal wedge was performed on #15.
The patient will have a final porcelain-metal teeth bridge made after the gums heal. Dental implants may also be placed in the upper right posterior. A bite plate is also necessary to try to mitigate the force of teeth grinding. Referral for pharmacological management of anxiety is also worthwhile.
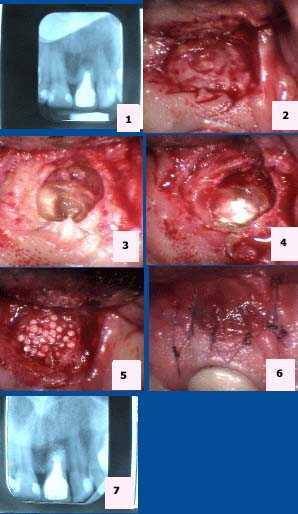
Dental radiographs x-rays show before and after an Apicoectomy root canal oral surgery for an upper front central incisor tooth #9. 1) Pre-op periapical x-ray showing periapical pathology. 2) Isolation of the apical area. 3) Exposure of the root apex. 4) Placement of MTA mineral trioxide aggregate. 5) Placement of Bioplant HTR hard tissue replacement. 6) 6-0 Vicryl stitches. 7) Post-op dental xray.
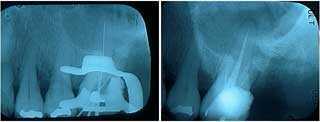
Dental x-rays show endodontic root canal retreatment of an upper left lateral incisor after a broken tooth crown came out. The adjacent central incisor tooth #9 will need to be extracted due to apical fracture. 1) Tooth #10 upper left lateral canal widened – cleaning and shaping – with an endodontic file. Old gutta percha is removed using chloroform solvent. A rubber dam clamp and rubber dam is in place on the tooth to maintain sterility. 2) Radiograph x-ray of an endodontic file marker used to measure the vertical depth of the root canal to the tooth apex. The prior gutta percha was not obturated – filled – to the root canal apex and the gutta percha had been left exposed to oral saliva after the dental crown fracture. 3) The Endodontist fills the root canal with new gutta percha – obturation – and a temporary post and a temporary tooth crown are placed. 4) The post-op final radiograph xray show the root canal obturation and the post space in preparation by the Endodontist for a cast gold post and core impression.
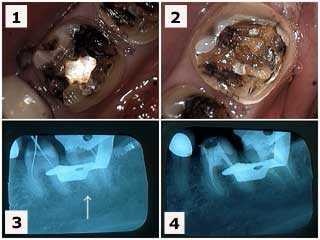
Before and after xrays radiographs show endodontic root canal retreatment of tooth #29 and initial root canal treatment of tooth #28. 1) The first dental x-ray shows the five teeth bridge that had dental cement leakage and the teeth abutments had dental caries after only 1 and 1/2 years. The patient said that she always felt tooth pain in #29 after the original root canal treatment was performed by her general dentist. 2) The second xray shows retreatment of #29 by an Endodontist – root canal specialist – revealed a second, previously undiagnosed and untreated second root canal within the tooth. A post space was created in this second canal after gutta percha obturation.
These dental radiographs xrays show how to extract a tooth from under a one piece 10 teeth fixed porcelain dental bridge. Before and after x-rays with pictures. Tooth root resection from under a large porcelain fused to metal teeth bridge can be accomplished with having to destroy and remove the bridge. 1) This radiograph xray shows the distal tooth abutment with a combined endo-perio lesion – root canal and gum infection. 2) Labial photo of the same tooth. 3) Dental radiograph x-ray following tooth root resection – the metal chad in the area of the extracted tooth abutment was later removed. 4) Labial photo following tooth extraction. This area could be filled in with dental bonding after wound healing. The occlusion teeth bite on the distal cantilever was reduced. It opposed a lower full arch bridge so that supra-eruption was not a concern. Subsequent dental treatment options include: i) sectioning and removal of the distal cantilever, ii) dental implants, or iii) reevaluate over time with the patient being informed to reduce function – chewing – in this area. We went with choice three given that the patient was a compliant elderly lady. This bridge is still functional seven years after completion of this dental repair.
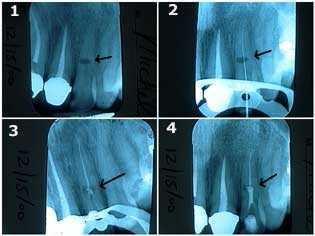
Radiographic x-ray series shows how to treat internal resorption in an upper left lateral incisor tooth. This patient said she had been in a horseback riding accident. 1) The initial dental xray shows an oval-shaped radiolucency in the middle of the tooth length; it is the site of the internal resorption. The patient was informed of the guarded long-term prognosis of the tooth. 2) & 3) These radiographs show that traditional root canal treatment was first performed by the Endodontist. The root canal space was cleaned and shaped, sterilized with NaOCL, and then filled with gutta percha obturation up to a point apical to the internal resorption. 4) The final x-ray shows Mineral Trioxide Aggregate placed into the area of the internal resorption and coronal to it. Keeping the MTA moist will give more working time for condensation of material.
A bitewing dental x-ray and two periapical radiographs show before and after root canal treatment for emergency premolar tooth pain. Root canal therapy, crown build-up and dental crown preparation were performed for both the molar and premolar teeth. The premolar is the focus in this series of xrays and pictures. The bitewing xray was used during dental diagnosis to get an early idea of the cause of the pain. Because it simultaneously shows the upper and lower teeth in one xray it also helps rule out referred pain from the opposing jaw. The before and after periapical xrays are used to look for a periapical pathology radiolucency and to confirm the final endodontic obturation root canal filling.
A bitewing dental x-ray and two periapical radiographs show before and after root canal treatment for emergency molar tooth pain symptoms. Root canal therapy, crown build-up and tooth crown preparation was performed for both the molar and premolar teeth. The molar is the focus in this series of dental radiographs x-rays. The bitewing xray was used during dental diagnosis to get an early idea of the cause of the pain. Because it simultaneously shows the upper and lower teeth in one x-ray it also helps rule out referred pain from the opposing jaw. The before and after periapical xrays are used to look for a periapical pathology radiolucency and to confirm the final endodontic obturation root canal filling.
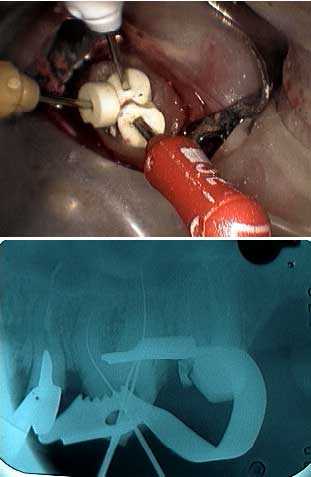
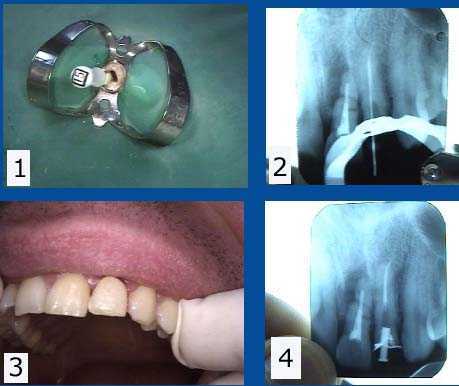
Pretreatment dental diagnosis xray of a maxillary central incisor tooth that needs an apicoectomy and retrograde filling to treat a failing root canal – periodical pathology. 1) Pre-op photo. 2) Radiograph x-ray of tooth #9 with a cast post and root canal filled with gutta percha to the apex. 3) Initial semi-lunar surgical incision exposes the bony fenestration. 4) The dental cyst is being pulled through the osteotomy with forceps. 5) Osseous preparation – drilling through the jaw bone – exposes the tooth root apex with the gutta percha – root canal filing material – visible. 6) Drilling preparation into the root apex to make room for the retrograde filling. 7) Retrograde filling material, Mineral Trioxide Aggregate, placed into the tooth root apex preparation. 8) Stitches.
Endodontic x-rays radiographs show an endodontic length measurement periapical xray and a final endodontic obturation periapical xray during the treatment of two adjacent mandibular molar teeth.
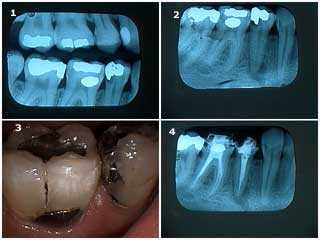
1) & 2) Pictures of teeth #’s 19 & 18 following removal of large, old silver dental fillings in a 38 year-old female patient who had been experiencing tooth pain. 3) Radiograph x-ray of the endodontic file length measurement. Note that the tooth calcification in the mesial root of #18 initially prevented instrumentation by the Endodontist. 4) Final endodontic obturation shows that the mesial root of #18 was located and treated. Chronic inflammation in the dental pulp due to the presence of large, old dental fillings can increase the difficulty of root canal treatment. Earlier endodontic root canal therapy should be considered in these situations.
Initial dental diagnosis bitewing and periapical radiographs x-rays of a patient who came with emergency tooth pain and two root canal treatment xrays. 1) & 2) X-ray of teeth #’s 19 & 18 showing large, old silver dental fillings in a 38 year-old female patient who had been experiencing teeth pain. Note the decreased size of the pulp chambers in these teeth. The bitewing xray was used during dental diagnosis to get an early idea of the cause of the pain. Because it simultaneously shows the upper and lower teeth in one xray it also helps rule out referred pain from the opposing jaw. 3) This x-ray shows the endodontic file lengths measurement. In this xray note the tooth calcification in the mesial root of #18 that initially prevented instrumentation by the Endodontist. 4) Final endodontic obturation radiograph shows that the mesial root of #18 was located and successfully treated. Chronic inflammation in the dental pulp due to the presence of large, old dental fillings can increase the difficulty of root canal treatment. Earlier root canal therapy should be considered in these situations.
X-rays of root canal therapy showing the initial file lengths measurement and then final endodontic obturation. These xrays are of a maxillary molar tooth in a 40 year old female. The first x-ray also shows the endodontic clamp placed around the tooth.
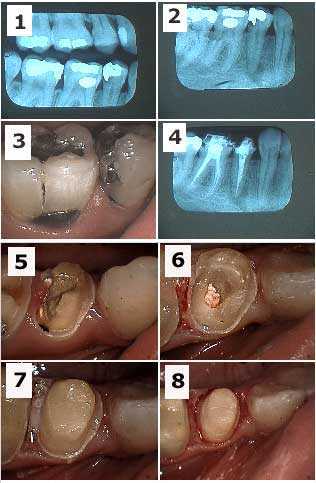
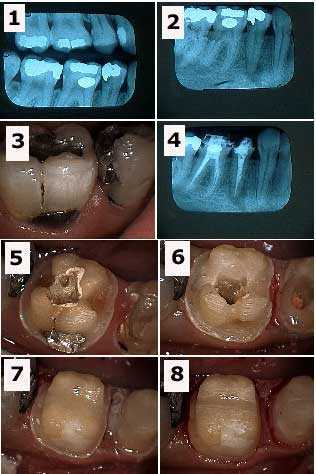
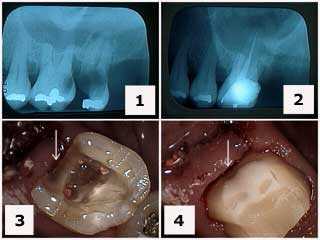
Before and after periapical dental radiographs x-rays of dental treatment of severe tooth pain symptoms in the maxillary left posterior. 1) The initial xray shows very large dental caries tooth decay in tooth #14 that is treatable and tooth #15 that needs tooth extraction. 2) X-ray following #15 tooth extraction and root canal treatment on tooth #14. Note the gingival extent of the tooth decay below the gums. 3) This picture shows tooth preparation drilling following root canal therapy and the removal of the distal tooth cavity. 4) Final tooth preparation of the composite crown build-up. Note how the distal tooth preparation extends gingivally towards the gum beyond the composite to tooth.
Radiographic diagnosis. 1) & 2) X-rays radiographs of tooth #14 show a large, old silver dental filling in a patient who had been experiencing tooth pain symptoms. In this x-ray note the decreased size of the tooth pulp chamber. 3) Radiograph xray of the endodontic file lengths measurement. Note that the calcification in the mesial root of #14 initially prevented instrumentation by the Endodontist. 4) Final endodontic obturation – root canal filling – shows that the mesial root of #14 was located and treated. Chronic inflammation in the tooth pulp due to the presence of large, old teeth fillings can increase the difficulty of root canal treatment. Earlier root canal therapy should be considered in these situations.
Emergency tooth pain symptoms in the mandibular right posterior quadrant. 1) This bitewing radiograph shows big teeth cavities – dental caries – in the second premolar and first molar and smaller dental cavities in both the second and third molars. This bitewing dental x-ray was also used to rule out referred pain from maxillary teeth. 2) In addition to the significant tooth decay noted above this periapical xray shows a large periapical pathology radiolucency around the tooth root apex of the second premolar. 3) Photo of the second premolar and first molar. 4) Radiographic post-op following root canal treatment of both teeth. The patient felt better immediately following this. Note: these teeth were treated following a careful differential diagnosis using dental radiographs xrays and clinical pulp vitality testing performed by an Endodontist. It would not be surprising, if in another patient, the pain came from a tooth with a less obvious cause.
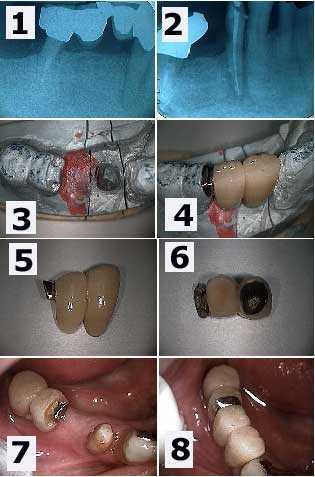
Cervical tooth decay and root canal infection is seen in the xray around a lower right first premolar tooth. 1) A large periapical radiolucency is seen in the diagnostic dental x-ray. Note in the radiograph that the distal abutment is the distal root of a first molar tooth that previously underwent hemisection. 2) Post op root canal treatment xray. The cervical tooth cavity can now be seen more easily. 3) The working model showing the preparation of the mesial part of the distal two-unit dental bridge. This tooth drilling – preparation – will allow a rigid connection to the new anterior teeth bridge being made. 4) The new dental bridge section in place on the working model. 5) & 6) Two pictures of the new bridge showing the distal attachment. 7) An intra oral photo which mirrors the working model view seen in 3). 8) The final result photo. This patient was content to see the gold occlusal rest. Otherwise, it could have been hidden under dental porcelain.
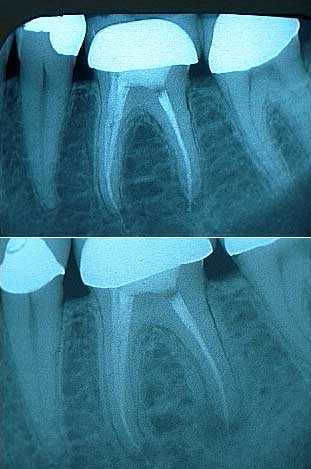
Before and after radiographs x-rays of a retreated molar root canal. 1) The post op radiograph x-ray of the initial root canal looks good. A little root canal cement can be seen extruding from the tooth root apices. 2) A two year follow up radiograph xray showed the development of an expanding periapical pathology radiolucency. This second xray shows the retreated molar and the periapical radiolucency at the time of the endodontic retreatment.
Radiographic comparison of the initial and final periapical radiograph x-ray of root canal retreatment of a maxillary second premolar tooth. The root canal filling material does not reach the apex of the tooth root in the initial xray but now does in the final radiographic view.
During root canal treatment – endodontics – the Endodontist needs to confirm that he/she is cleaning and shaping the tooth root canal to the full length of the tooth. The result should not be longer or shorter than the length of the tooth. The Endodontist will frequently use an electronic tooth root apex locator in conjunction with dental xrays radiographs to confirm this measurement. The Endodontist will always want a pre-treatment x-ray to help radiographic diagnosis and a final treatment x-ray to confirm that the root canal filling – endodontic obturation – is at the correct length within the root canal space.
Three endodontic files placed in a maxillary molar to verify the correct lengths in the radiograph. During root canal treatment – endodontics – the Endodontist needs to confirm that he/she is cleaning and shaping the tooth root canal to the full length of the tooth. The result should not be longer or shorter than the length of the tooth. The Endodontist will frequently use an electronic tooth root apex locator in conjunction with dental xrays radiographs to confirm this measurement. The Endodontist will always want a pre-treatment x-ray to help radiographic diagnosis and a final treatment x-ray to confirm that the root canal filling – endodontic obturation – is at the correct length within the root canal space.
1) Tooth #11 pre-operative radiographic x-ray film shows the periapical pathology radiolucency. 2) The final root canal treatment radiograph xray shows the gutta percha obturation reaching the apex of the tooth root. This emergency patient presented with symptoms of severe tooth pain and swollen gums in the mucobuccal fold.
Before and after radiographs x-rays of severe periapical pathology around the mesial and distal tooth roots of #30 leading to tooth extraction. This patient presented with severe tooth pain and swollen gums and cheek. The dental diagnosis periapical x-ray shows a large periapical radiolucency consistent with root canal failure. Some Oral Surgeons consider that a periapical radiolucency that is larger than five millimeters as seen in an xray is more likely to subsequently need an apicoectomy after endodontics root canal treatment. This tooth was too far gone to save. The after radiograph shows the extent of the damage to the surrounding jaw bone. Regular dental checkups and x-rays would have prevented the extent of the damage by earlier intervention. Photo 1 of 3
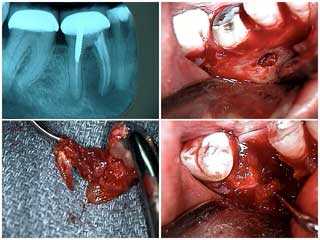
Tooth extraction of a mandibular molar due to severe periapical pathology. 1) Radiograph x-ray shows a large periapical pathology radiolucency around both the mesial and distal tooth roots. 2) Buccal fenestration around the mesial root following a vertical incision and periodontal flap performed by an Oral Surgeon. 3) The extracted mesial root with the dental cyst pathology that was sent for biopsy. 4) The tooth extraction site. Radiographic diagnosis during routine dental checkups could have diagnosed this problem earlier and this tooth could possibly have been saved. Routine checkup xrays are worthwhile but should not be overused. Photo 2 of 3
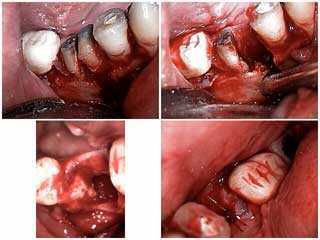
How to tooth extraction of of a mandibular molar due to severe periapical pathology. More pictures of the dental treatment shown above. 1) Sectioning of the mesial and distal tooth roots. 2) Removal of the mesial root. 3) & 4) The tooth extraction site. Photo 3 of 3
In this dental x-ray the maxillary right central incisor shows complete obliteration of the canal from calcification secondary to a history of trauma. Note discoloration of coronal portion of tooth. This is a result of the breakdown of blood in the pulpal chamber and the leaching of hemosiderin into the dentinal tubules. A periapical radiograph xray should be taken if one tooth appears to be a different color – usually darker – that the others.
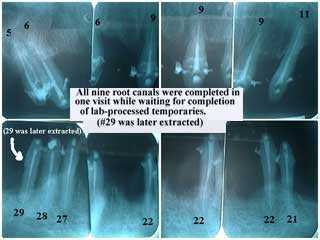
These periapical radiographs xrays show the final endodontic obturation for nine teeth that received root canal treatment in one visit. The Endodontist performed these root canals while a Cosmetic Dentist worked with a dental laboratory technician to create the fixed provisional temporary dental crowns the patient was to receive later that same day. Tooth #29 was later extracted.
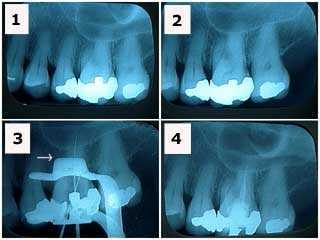
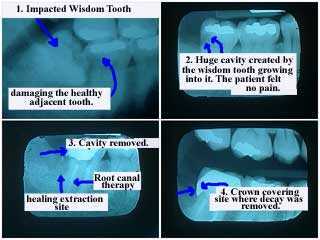
These film periapical radiographs show how an impacted wisdom tooth damages the healthy adjacent tooth. A large tooth cavity – dental caries – was created by the wisdom tooth growing into it. The patient did not feel tooth pain symptoms. The dental treatment is shown using this xray series. In the final x-ray the completed root canal and dental crown can be seen; the dental crown covers the distal area where the tooth decay was removed.
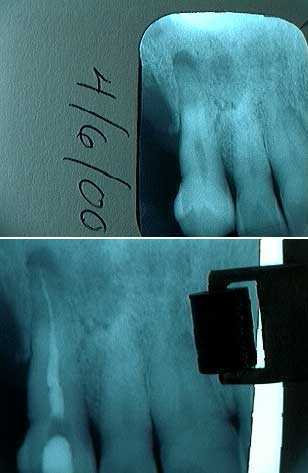
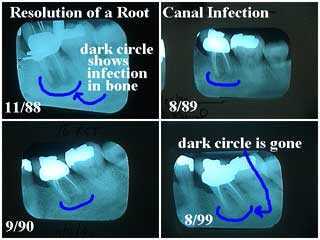
Resolution of an endodontic root canal periapical radiolucency seen in dental x-rays radiographs over 11 years. The periapical radiolucency – the dark circle at the tooth root apex – is radiographic evidence of periapical pathology PAP – root canal infection. The first x-ray shows the initial root canal treatment performed in November 1988. The second and third xrays show how jaw bone is beginning to grow and fill in the area of the original PAP. Xrays measure density: the darker something is on an x-ray the less dense it is and the whiter something is on an xray the more dense it is. Bone loss from infection therefore appears darker while bone regrowth appears whiter. The final xray taken in August 1999 shows the dark circle is completely gone indicating that bone has grown back into the area where infection have previously destroyed it.
Root canal post-op radiographs x-rays of a dental reconstruction smile makeover. 14 of the 15 root canals seen in these xrays were completed by the Endodontist during one visit.
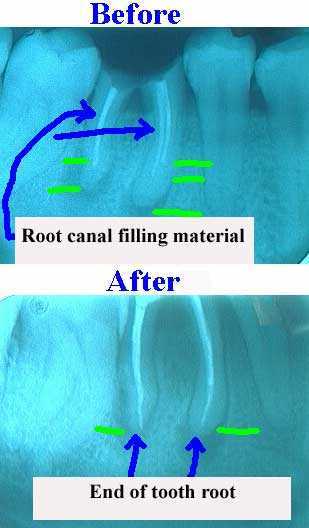
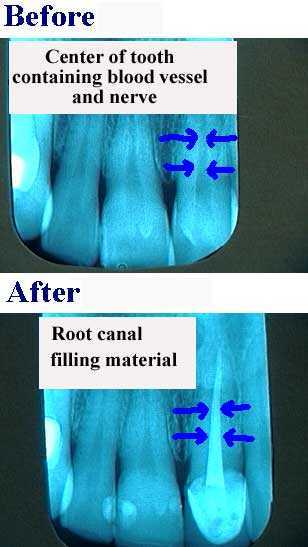
Before and after xrays of Root Canal ReTreatment. Endodontic obturation – the root canal filling material – should extend to the end of the tooth root when properly performed. The initial dental xray clearly shows the root canal filling material ending far short of the end of the tooth. The retreatment x-ray shows a significant improvement with the root canal filling material ending properly at the end of the tooth root. Patients should ask to see their post-op x-rays! It is not too difficult to judge good root canal from bad with just a little practice!
Root Canal ReTreatment before and after xrays radiographs. Poor quality root canal therapy in the top x-ray does not show root canal filling material to the end of the tooth root. This allows bacterial leakage and infection that can frequently result in symptoms of tooth pain and/or swollen gums. The retreatment xray shows a significant improvement with the root canal filling material ending properly at the end of the tooth root. Patients should ask to see their post op root canal x-rays! It is not too difficult to judge good root canal from bad with just a little practice!
Root Canal Therapy Initial Treatment x-rays for tooth pain symptoms. These before and after root canal x-rays or radiographs again clearly show that the root canal filling material should extend to the end of the tooth root when therapy is properly performed. Got it? Now go look at your dental x-rays! General Dentists are legally allowed to perform root canal treatment but Endodontists do nothing else so they get a lot more “practice” and are usually able to do it better and faster.
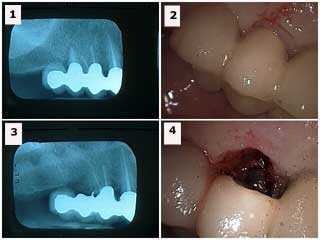
A dental xray can be used to locate the origin of a draining fistula. This can aid dental diagnosis. Gutta percha can be gently placed into a draining fistula without anesthesia and a radiograph x-ray taken. The gutta percha will end at the source of the infection. The gutta percha is NOT shown in this root canal x-rays.
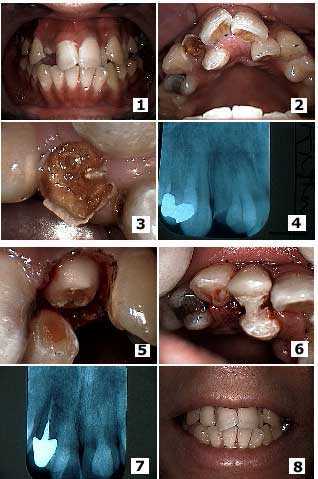
Before and after pictures and dental radiographs x-rays of a complex dental treatment of a broken tooth lateral incisor with severe tooth decay adjacent to a palatally-displaced supernumerary tooth. 1) – 2) Initial presentation. 3) Close up photo 4) Initial radiograph x-ray. 5) The same tooth after gum surgery and initial tooth preparation. 6) Placement of the temporary dental crown. Note that acrylic was extended from the temporary crown on the lateral to the supernumerary tooth to provide initial stability of the temporary until root canal treatment was completed and a cast post and core was placed. 7) X-ray of the final root canal therapy, cast post and core and dental crown. 8) Final result photo.
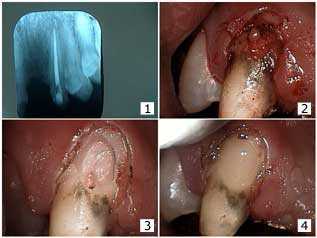
Initial xray for a patient seeking repair of a dental bridge. 1) Root canal x-rays after root canal therapy. The root canal itself did not seem subject to external resorption. 2) Gingivectomy. Note the still unusual look of the facial tooth decay. 3) Following dental caries removal. Note the communication to the gutta percha. 4) The tooth bonding restoration.
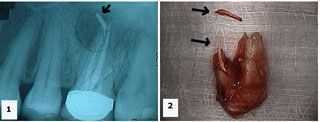
Diagnosis radiograph of a hopeless tooth. 1) X-ray shows an upper first molar with gutta percha extruded into a large radiolucent area. 2) Palatal photo of the extracted tooth shows the extent of the gutta percha extrusion. The extra fragment shown is also gutta percha. [jm-o]
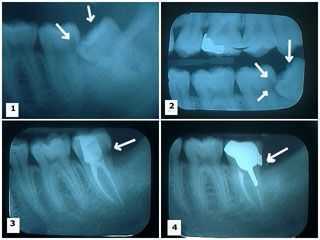
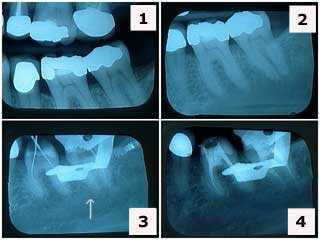
Radiographic explanation of the rationale for wisdom tooth extraction: damage to the adjacent second molar. 1) – 2) Two x-rays showing a lower wisdom tooth impacted on an angle and pushing into the adjacent second molar causing a large cavity. 3) X-ray shows the wisdom tooth was removed and the second molar following root canal therapy with the large distal cavity still present. 4) Xray shows cast gold post and core and dental crown in place. Note the distal crown margin completely covers where the distal tooth cavity was removed.
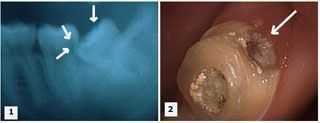
Rationale for wisdom tooth extraction explained in a dental radiograph and photo: damage to the adjacent second molar. 1) X-ray shows a lower wisdom tooth impacted on an angle and pushing into the adjacent second molar causing a large tooth cavity. 2) Tooth decay is present in the distal area of the second molar. Temporary dental filling material is visible in the occlusal opening following root canal treatment. This patient had experienced severe tooth pain symptoms. It could have been avoided with regular dental checkup xrays and following a recommendation of timely wisdom teeth extractions.