Top 12 Ways People Can Become Educated Dental Consumers
December 28, 2014 6:30 pmTop 12 Ways People Can Become Educated Dental Consumers
by Dr. Jeffrey Dorfman*
People who visit a dentist should become educated about how to differentiate a good from bad dentist and how to differentiate good from bad dentistry. One can certainly search online for dentist reviews and/or learn about malpractice claims on various websites of dubious quality. People may also visit the dental office and read academic degrees and membership in professional organizations that are framed on the walls. This is totally inadequate. This article is an insiders view to dentistry written by a master clinician who has over 20 combined years of professorships at NYU and Columbia dental schools and who is also director of Advanced Dental Education at The Center for Special Dentistry® for almost 30 years. The dentistry he has personally seen and the stories he has personally heard from former students who are now in practice around the country is scary and sad.
One of the first questions a prospective dental patient should learn is how many years has the dentist been in practice? If the dentist is young is he/she working in an established practice with older more experienced dentists who appear to be interested in actual patient care? Or instead does the practice appear to be run by a non-dentist office manager that is owned by an absentee dentist? Is the office clean and do the treatment rooms appear to be sterile? Are instruments and dental drills removed from sealed clear plastic bags that have been subjected to real sterilization or does it appear that disinfection (not sterilization) is your best hope? Is fresh plastic wrapped around everything that might be touched? Do the dentist and staff wash their hands and put on fresh gloves, mask and eye protection before the procedure begins?
A good dentist is trustworthy, intelligent and knows his/her skill limitations. Trust implies that the dentist is looking out for the best interest of the patient instead of personal economic gain. Trust is something one feels intuitively, and given the lingering Great Recession, people should be even more aware that trust is something that should be earned before it is granted. Does the dentist photo document the work they plan to perform on you and if so are they willing to email those photos to you? Are x-rays taken every six or 12 months during teeth cleaning visits as allowed by your insurance plan? This is very common and is frequently performed much more often than necessary to help dentists recoup income lost by participation in managed care insurance plans. Are x-rays taken immediately by office staff – possibly under the direction of the office manager – instead of after careful consideration by the treating dentist?
Is significant treatment suddenly being suggested or even pushed? Is a thorough explanation offered for the need for such treatment? Do you think too many cavities are being discovered and that many of them need crowns instead of fillings? Is other possibly less lucrative treatment being ignored? For example, gum disease is commonly under diagnosed and under treated. Failure to diagnose and treat gum disease is a significant cause for malpractice claims. Don’t think you can drive to your dentist in your new Mercedes and talk about your family ski trip to Aspen and then expect him/her to be happy to accept your in-network managed care plan payments. Dentists and doctors are getting squeezed by the Affordable Care Act and many need alternative revenue streams while they also reduce costs. Consider participation in an out-of-network Fee For Service (FFS) plan rather than an in-network Preferred Provider Organization (PPO) plan if you can afford to do so. The significant difference in those fees is not made up by the insurance company but instead comes out solely from the dentist’s bottom line. That has to directly impact your treatment in terms of skills, materials and time.
An intelligent dentist need not be Ivy League educated. Instead he/she should possess the innate ability to make an accurate diagnosis and then, like a chess grandmaster, be able to see all possible treatment options before them. Surprisingly, the ability to properly diagnose a patient and see all subsequent treatment options can vary as widely as the skills one can notice watching 12 year olds playing Little League. Some kids can clearly play ball while others will probably give up at the end of the season; the majority of the Little Leaguers demonstrate middling skill. Dentistry is no different.
A good dentist should possess the communication skills to clearly articulate the diagnosis and also be willing to spend the time necessary to discuss treatment options. Treatment time, benefits and risks of treatment and cost should be discussed for all treatment options. Upon reaching a mutually agreed course of treatment a “treatment plan” should be written and signed. Ideally this should all be done with the treating dentist but it may not be possible in this age of managed care; frequently office staff are delegated this task. The question is then what is the qualification of the office staff to have this discussion and make appropriate treatment recommendations? It could be argued that anyone other than the dentist making treatment plan decisions with a patient is actually practicing dentistry without a license.
So let’s assume we have found the perfect honest and intelligent dentist who has a reasonable number of years experience and the office is spotless. The next question is do they have “hands?” Does the dentist possess the requisite eye-hand skills to carefully perform the dentistry desired by their own heart and mind? Let’s not forget the good student who becomes a dentist because it offers a wonderful lifestyle but they never considered the fact that they have difficulty replacing a light bulb at home. We all know those types of people and sadly many of them become dentists. Does the dentist discuss hobbies like playing a musical instrument, painting or sculpture, carpentry or playing sports at a higher level of skill? These hobbies are sought out by dental schools as one measure of an applicants potential eye-hand skills.
If we discover that this perfect dentist used to be a studio musician with Pearl Jam then the next question is time. Does the office schedule allow the dentist the necessary amount of time to carefully perform this dentistry or must they expeditiously run off to the next patient. Good dentistry requires time – and a little extra time if the initial work doesn’t turn out quite right and something needs to be redone. About 10% of my dentistry runs 50% longer than expected so I build that time into every appointment – just in case I need it. And while we are discussing time, consider this: the most common reason people don’t visit the dentist is because of fear. Novocaine takes time after the injection to get you numb. In my office I typically allow 15 minutes after the injection before I begin treatment in the lower jaw. Think of novocaine like a glass of wine. If you drink a glass of wine after work with your spouse you probably don’t immediately feel the relaxing effect immediately after the first few sips; it takes a few minutes.
Another question is whether an honest and intelligent dentist with good hands is capable of performing most specialty work himself/herself. In my opinion the answer is generally no. A skilled dentist may be reasonably skillful in one or several areas of specialty dentistry but a given specialist does nothing other than that specialty procedure all day long. How can you compare? The question then is the dentist willing to appropriately refer dentistry to specialists and thereby either lose, or have to share, the higher fee specialty dentistry? In many cases dentists perform their own specialty dentistry with results that are less than ideal for the patient.
So now you visit your perfect dentist who is sterile, honest, intelligent and has good hands. He photo documented all your treatment and appropriately referred you to, for a example, an endodontist (root canal specialist) before he proceeds to make your porcelain crown. All crowns are the same – aren’t they? Surprise, porcelain crowns can vary drastically in how they are made: the material composition, the skill and artistry of the individual porcelain ceramist, dental laboratory and even the country in which they are made. Many crowns made for patients in the USA are now made in China. Remember the problem with Chinese toothpaste and drywall a few years ago? Imagine that permanently cemented in your mouth. Then let’s hope it looks nice because it takes serious skill – and yes time – to make crowns fit well and look natural.
After 29 years of dental practice it still surprises me when potential patients call our office to ask the cost of a procedure as if showrooming via telephone is a good way to choose a doctor. “No, we are not a managed care dental office.”
*Dr. Jeffrey Dorfman is Director of The Center for Special Dentistry® and publisher of NYCdentist.com, a website containing over 4,400 pages of original free content.
This is an Example of Bad Dentistry
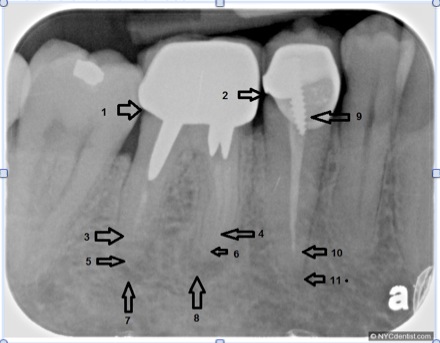
Was this the result of a dentist who was untrustworthy, unintelligent and who lacked “good hands” and the time to perform good dentistry?
Did this dentist perform the root canal specialty work himself/herself? Where were the crowns made?
1) There is a cavity under this crown. 2) There is a cavity under this adjacent crown. The root canal filling (arrows 3, 4 & 10) does not extend to the end of the tooth root (arrows 5, 6 & 11). 7) & 8) X-ray evidence of an active root canal infection in the jaw. Pain in this tooth was the reason for this new patient visit. He thought his dentist was his friend. 9) A poor-fitting prefabricated post. The molar tooth will likely need extraction and replacement with a dental implant and new crown. The premolar tooth will need root canal retreatment, a new post, possible gum surgery and a new crown.
Categorised in: Dr. Dorfman Says
This post was written by Dr. Jeffrey Dorfman